
|
BB © 2013 |

By Judith Elaine Halek
Photos and Article Copyright @ 2013 Judith Elaine Halek
Being a good dad is like being a good husband–learn as you go and do the best you can. One thing prospective fathers should keep in mind is this: a couple-focused pregnancy provides both a healthier pregnancy and birth experience and is a time when all three parties bond. Although fatherhood is probably the most important role a man will play in his lifetime, many men have been culturally and emotionally separated from pregnancy and the childbearing process.
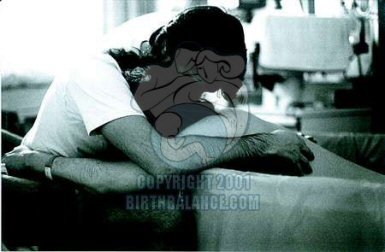
As an observer at many births, my grandest observation is the remarkable change that takes place in men (whether the actual father or partner, a friend, brother or family member) while assisting the labor and birth. One father commented, “I have a newfound respect for my wife. I don’t think I could have ever done what she did, go through what she went through to have our child.”
During a baby’s birth, the father’s presence can markedly alleviate a mother’s pain and anxiety, and it certainly enhances his experience of the birth. It is crucial the mother not feel alone during this strenuous time. Many studies have shown that infants recognize and respond to voices they hear in the womb, therefore it is important to maintain a modicum of peace, tranquility and communication at all times.
One father who acted distant and angry during the labor and birth of his child finally let go of most of his defenses when I challenged, “Can we put the weapons down and let the egos go so we can help your child enter a place of welcome and peace?” By the time the baby was actually out daddy had softened immeasurably.
Those of you who have witnessed a birth know what I’m talking about. A sacred transformation takes place that crosses beyond the boundary of mere words.
My extensive work assisting people make the informed choice to birth babies in water and/or use water labor instead of the traditional “drug the mother” syndrome has brought both myself and the clients’ experience to newer, loftier heights. I have become very curious about fathers’ reactions and level of participation. I began to keep data–who initiated the idea and when the decision was made, were fathers able to support their partners during preparation, and did they clean up after the event?
It was important for me to know exactly what these new fathers would say about their waterbirth experience to other prospective dads. I set about doing this by interviewing six waterbirth fathers. They ranged from thirty to sixty years old with Indian, Italian, Hispanic and African American backgrounds.
 When I asked the father why he chose to attend the labor and birth of his partner, the responses were uplifting. “Why not?” said a new daddy, “It’s my child as well. To me it was a moment getting to know and get closer to my wife. I can assure you, it did. It took the relationship to another level. Relationships are a collection of experiences and it’s brought us closer together. Forget the candlelight dinners guys, you can’t compare it and it may happen only once or twice in your life. Don’t miss it.”
When I asked the father why he chose to attend the labor and birth of his partner, the responses were uplifting. “Why not?” said a new daddy, “It’s my child as well. To me it was a moment getting to know and get closer to my wife. I can assure you, it did. It took the relationship to another level. Relationships are a collection of experiences and it’s brought us closer together. Forget the candlelight dinners guys, you can’t compare it and it may happen only once or twice in your life. Don’t miss it.”
Another father told me,” I felt it would be a good thing to see a baby born into this world. Doctors see this all the time, why can’t I?”
One man said, “I wanted to be part of it. We are a team. I was also curious to see the whole process. I’m in my thirties. Most of the guys in my generation are really into supporting their partners as opposed to older generations who might not be so interested in seeing the whole experience.”
When asked whose idea it was to have the waterbirth, most men responded, “both partners.” One father commented, “We were unhappy with conventional births. When we heard there was a more gentle, drugless approach to having a baby we went to a waterbirth educator and realized it was more normal to have the baby in water than the air. My wife’s obstetrician told us about a waterbirth educator. When we saw the videos I was really more supportive of doing the birth this way. At first I had to talk my wife into it. But that didn’t take too long.”
Another father told me, “The midwife suggested it. My wife was very open to it so I had no objections. We’d had three babies the traditional air birth. My second wife and I were having our fourth when we saw pictures of water babies. They looked so much calmer and happier. That’s when we decided to have our next child underwater.”
When asked about concerns or fears regarding this alternative method, one father replied, “No concerns. The water looked less traumatic and more comfortable for my wife and baby. It was something completely new to us.” Another dad added, “We had only heard of it two to three weeks prior to the birth of our child. It was a little nerve-racking, but I had no specific concerns.”
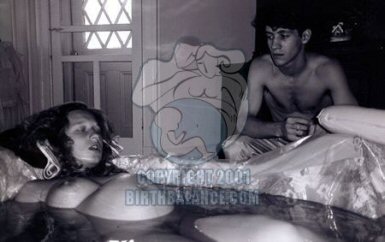
It was the father’s choice to enter or not enter the birth pool. One dad had a cold and didn’t think going in was a wise decision; others just felt a little overwhelmed. One excited father who did enter the pool said, “This goes to show how things can change. I thought I wouldn’t go in, but I was in the water ten minutes before my wife. I didn’t want to miss a moment of the birth. It was OK. I was behind my wife. I could hear the doula and the documentarian say, ‘Here comes the head.’ When the moment came, I was crying like a baby. I was totally overwhelmed!”
When queried about how important a part the water played, one father responded, “Vital–the only thing that prevented her from getting drugs!” Another stated, “The water was like a lifeline for her, something she could hold onto even if she didn’t use it very much until the birth. Just having it was her security.”
Preparation for a waterbirth means going to a waterbirth educator, getting an OK from the medical caregivers and institutions, looking at videos and pictures, ordering a tub, and lots and lots of talking to each other. If your facility does not supply a tub, you’ll need to rent one. Once done you must make contact with the hospital or birth center maintenance staff to ensure that the hot water hose adapters match the water faucets. Prior to the labor you will want to actually set up the tub.
Filling up the tub is optional but timing is everything, so get an idea from the staff how long your tub might take to fill. Knowing this relieves both parents of undue stress.
One of the most important elements mentioned by all six men was the hiring of a labor support specialist or labor doula. This is a person specializing and certified in assisting couples during their labor and birth. The doula attends the mother and baby while the father is busy with the tub before and after the birth. It is an added bonus if the doula is experienced in the waterbirth arena. She can give helpful tips on when to utilize the water and when it’s unnecessary.
One father advised, “Let the midwife and doula, if there is one, do their job. This is the best way to go if you don’t want to see your wife suffer.”
If you are considering the unique joy of waterbirth, make sure you employ a doula who is a team player. She should be open to allowing your full participation. Knowing and trusting her methods can really relieve the pressure. Though it may take some time, get the medical establishment to support you in your choice. Next, seek out a waterbirth educator or a labor specialist interested in waterbirth. Watch as many videos as possible and above all, be patient. Talk to people who have had this experience. Remember, knowledge is power. Make a choice to become intimately involved in one of life’s greatest moments. You won’t regret it.

 scooper for scooping out fecal and birth matter released in the water during labor or birth, they purchase one from a local pet store, sterilize it and wrap it in a plastic Ziploc. Urinating in the water is fine. Urine is sterile and clearing the bladder will make room for the babies’ head to dip down. I suggest, however, that all labor attendants in the water use the bathroom facilities.
scooper for scooping out fecal and birth matter released in the water during labor or birth, they purchase one from a local pet store, sterilize it and wrap it in a plastic Ziploc. Urinating in the water is fine. Urine is sterile and clearing the bladder will make room for the babies’ head to dip down. I suggest, however, that all labor attendants in the water use the bathroom facilities.





 ~
~ When one takes rolaids, it is COUNTER PRODUCTIVE to the absorption of the iron in the body. Rolaids is an ANTACID, (not acidic) and you NEED acid to absorb the iron in your body. So, you are just canceling out the iron supplement each time a rolaid is taken. It doesn’t matter if one takes one or ten…IT IS NOT GOOD! Research shows if a pregnant woman has to choose between chalk and rolaids, the more favorable choice is the chalk. It doesn’t have the antacid element to it. STOP rolaids immediately if your doctor has suggested this as a solution away from the chalk.
When one takes rolaids, it is COUNTER PRODUCTIVE to the absorption of the iron in the body. Rolaids is an ANTACID, (not acidic) and you NEED acid to absorb the iron in your body. So, you are just canceling out the iron supplement each time a rolaid is taken. It doesn’t matter if one takes one or ten…IT IS NOT GOOD! Research shows if a pregnant woman has to choose between chalk and rolaids, the more favorable choice is the chalk. It doesn’t have the antacid element to it. STOP rolaids immediately if your doctor has suggested this as a solution away from the chalk. Floradix is a liquid formula that will help to enhance the iron absorbtion in one’s body when eating iron rich foods.
Floradix is a liquid formula that will help to enhance the iron absorbtion in one’s body when eating iron rich foods. 1. Ferrous Phosphate: 6X or 12X strength, take 1-4 times per day, 4 pellets. This very useful cell salt is known as the “oxygen carrier”. It has the ability to carry oxygen to all the cells of the body for use in conversion to energy.
1. Ferrous Phosphate: 6X or 12X strength, take 1-4 times per day, 4 pellets. This very useful cell salt is known as the “oxygen carrier”. It has the ability to carry oxygen to all the cells of the body for use in conversion to energy. The 12 Tissue/Cell Salt Combination As the name implies, this is a combination of all 12 salts in a single tablet. This combination can be used daily in much the same way as you would take a vitamin or supplement. To treat specific conditions, however, select one of the single salts listed above. RECOMMENDED POTENCY – 6X is the most widely used potency. These are all the different MINERALS combined into the 12 Tissue/Cell Salts.Calcarea Fluoricum Calcarea Phosphoricum Calcarea Sulphuricum Ferrum Phosphoricum Kali Muriaticum Kali Phosphoricum Kali Sulphuricum Magnesia Phosphoricum Natrum Muriaticum Natrum Phosphoricum Natrum Sulphuricum Silicea (Silica)
The 12 Tissue/Cell Salt Combination As the name implies, this is a combination of all 12 salts in a single tablet. This combination can be used daily in much the same way as you would take a vitamin or supplement. To treat specific conditions, however, select one of the single salts listed above. RECOMMENDED POTENCY – 6X is the most widely used potency. These are all the different MINERALS combined into the 12 Tissue/Cell Salts.Calcarea Fluoricum Calcarea Phosphoricum Calcarea Sulphuricum Ferrum Phosphoricum Kali Muriaticum Kali Phosphoricum Kali Sulphuricum Magnesia Phosphoricum Natrum Muriaticum Natrum Phosphoricum Natrum Sulphuricum Silicea (Silica) Spinach is a source of non-heme iron, which is usually found in vegetable sources. Unlike heme iron found in animal products, non-heme iron is not as bioavailable to the body.
Spinach is a source of non-heme iron, which is usually found in vegetable sources. Unlike heme iron found in animal products, non-heme iron is not as bioavailable to the body.

 ~
~ Of course, I am in favour of the abolition of electronic fetal monitoring but it would be far more uplifting if this was being done for some sort of health improvement and not just more ways to cover butt in court.
Of course, I am in favour of the abolition of electronic fetal monitoring but it would be far more uplifting if this was being done for some sort of health improvement and not just more ways to cover butt in court. One of the midwife “tricks” that we were taught was to ask the mother’s shoe size. If the mother wore size five or more shoes, the theory went that her pelvis would be ample. Well, 98 percent of women take over size five shoes so this was a good theory that gave me confidence in women’s bodies for a number of years. Then I had a client who came to me at eight months pregnant seeking a home waterbirth. She had, up till that time, been under the care of a hospital nurse-midwifery practise. She was Greek and loved doing gymnastics. Her eighteen-year-old body glowed with good health, and I felt lucky to have her in my practise until I asked the shoe size question. She took size two shoes. She had to buy her shoes in Chinatown to get them small enough—oh dear. I thought briefly of refreshing my rusting pelvimetry skills, but then I reconsidered. I would not lay this small pelvis trip on her. I would be vigilant at her birth and act if the birth seemed obstructed in an unusual way, but I would not make it a self-fulfilling prophecy. She gave birth to a seven-pound girl and only pushed about twelve times. She gave birth in a water tub sitting on the lap of her young lover and the scene reminded me of “Blue Lagoon” with Brooke Shields—it was so sexy. So that pelvis ended the shoe size theory forever.
One of the midwife “tricks” that we were taught was to ask the mother’s shoe size. If the mother wore size five or more shoes, the theory went that her pelvis would be ample. Well, 98 percent of women take over size five shoes so this was a good theory that gave me confidence in women’s bodies for a number of years. Then I had a client who came to me at eight months pregnant seeking a home waterbirth. She had, up till that time, been under the care of a hospital nurse-midwifery practise. She was Greek and loved doing gymnastics. Her eighteen-year-old body glowed with good health, and I felt lucky to have her in my practise until I asked the shoe size question. She took size two shoes. She had to buy her shoes in Chinatown to get them small enough—oh dear. I thought briefly of refreshing my rusting pelvimetry skills, but then I reconsidered. I would not lay this small pelvis trip on her. I would be vigilant at her birth and act if the birth seemed obstructed in an unusual way, but I would not make it a self-fulfilling prophecy. She gave birth to a seven-pound girl and only pushed about twelve times. She gave birth in a water tub sitting on the lap of her young lover and the scene reminded me of “Blue Lagoon” with Brooke Shields—it was so sexy. So that pelvis ended the shoe size theory forever.






