~ 

 ~
~
Whether you are pregnant, a medical or non medical caregiver, post partum doula, baby nurse or teacher, you know that immune systems are compromised during the winter months. Flu pandemics are valid concerns. Pregnant women are more vulnerable because their immune systems are suppressed during pregnancy so that their bodies don’t reject the baby.
The following piece is from Midwife: Gloria Lemay with her research on the H1N1 vaccine as well as preventative suggestions:
 “The publicity for the H1N1 vaccine is pervasive. Pregnant women are being focused on as a group that should be first in line to receive the vaccine. The fact that the vaccine is highly experimental and contains mercury (thimerosol preservative) has not escaped pregnant women and childbirth workers.” (I, Judith, coordinator of this blog, have read on some sites one can request to have the vaccine WITHOUT the thimerosol preservatve in it. They may not have it at your clinic or doctor’s office.)
“The publicity for the H1N1 vaccine is pervasive. Pregnant women are being focused on as a group that should be first in line to receive the vaccine. The fact that the vaccine is highly experimental and contains mercury (thimerosol preservative) has not escaped pregnant women and childbirth workers.” (I, Judith, coordinator of this blog, have read on some sites one can request to have the vaccine WITHOUT the thimerosol preservatve in it. They may not have it at your clinic or doctor’s office.)
“When the public is polled about who will take the H1N1 vaccine, almost half the population say they will refuse it. Thanks to the internet and other people-centered media, the experts who disagree with this mass population vaccine program have gotten the message out that the vaccine is far more dangerous than the disease.
What can a pregnant woman do to protect herself from H1N1 if she refuses the vaccine program?
Again, the media suggestions of sneezing into your sleeve and washing your hands with toxic sanitizers don’t get to the heart of the issue. We all need to take charge of having the best immune response possible so these suggestions, although directed at pregnant women in the fall of 2009, are good lifestyle advice for everyone.
1. Go to bed at 10 pm or earlier in a very dark room. Healthy sleep is important. Get rid of lighting in the bedroom (nightlights, electronic clocks, etc.)
2. Change your bedding and towels once a week.
3. Eat foods high in Vitamin C. Grapefruit, oranges, kiwi fruit and red peppers. Get used to these fruits as dessert.
4. Eliminate white sugar and flour from your diet.
5. Eliminate caffeine (coffee, tea, colas, chocolate).
6. Buy a wool scarf and mittens and be sure to bundle up warmly when you go out into the cold. Scarves help maintain your body heat and can be unwrapped and stuffed into your pocket when you go into a store or office building to adjust your warmth level.
7. If you feel the first tickle of a cold or sore throat, cancel everything and go straight to bed with hot herbal tea and a bag of grapefruit. Nip it in the bud with rest, Vitamin C and inner warmth.
8. Here’s a link to herbs that are safe in pregnancy. Learn to love your herb teas.
9. Slow down and enjoy your pregnancy. This is a special time in your life. Say “no” to overbooking yourself and consider quitting work earlier than you planned.
10. Keep your partner healthy, too.
Your baby will thank you for adopting these measures and you’ll have more energy, too. The first 3 days are the hardest and, then, you’ll love this routine. I’m sure the comments will have lots more tips, too, read on.”
________________________________________________________________________
One commenter who worked with twins said this, “I work with a lot of twins who are usually preemies and so the parents tend to be extremely concerned about germs and have had the vaccine pushed on them by their doctors. I have had a bad vaccine reaction in the past as an adult and so don’t get vaccinations but what I do is to take the homeopathic version of the vaccine which is called Influenzinum. It changes every year according to the new strain of the virus and this year also includes the homeopathic version of the H1N1 vaccine. I take it once a week October through June and am rarely sick even though I do not get good sleep. (I work mostly nights.) To get it just call your local homeopath (you won’t need a consultation) or you can order it online here:
http://drfeder.com/index.php?page=shop&action=viewProduct&itemID=124
This is where I get mine. When I tell my clients I am doing this they have all been fine with it. I think they just want to know I am being proactive about my and therefore their children’s health.”
 Influenzium: Winter Tonic is a homeopathic combination of flu types from 1918 to the present. The combination of flu types is then combined with ingredients that help strengthen the immune system during the cold and flu season. Winter Tonic (4 pellets) can be taken once a week during the cold and flu season. For children a and adults. Contains: Influenzinum; Otitis; Sinusitisitum; Grippe; (All 6C) 4 dram bottle, 400 pellets Produced by NHP
Influenzium: Winter Tonic is a homeopathic combination of flu types from 1918 to the present. The combination of flu types is then combined with ingredients that help strengthen the immune system during the cold and flu season. Winter Tonic (4 pellets) can be taken once a week during the cold and flu season. For children a and adults. Contains: Influenzinum; Otitis; Sinusitisitum; Grippe; (All 6C) 4 dram bottle, 400 pellets Produced by NHP
Check out Dr Feder’s website at: www.dr.feder.com in general for his information on alternative immune booster suggestions. He also has an interesting article on H1N1 (Swine) Flu:
http://drfeder.com/index.php?page=articles&action=viewArticle&articleID=295
Three things that can’t hurt and may well help: Vitamin D-*3*, up to 10,000 IUs a day if the flu is coming on. Otherwise, 2,000 – 4,000 daily as a preventative. Vitamin D is not given in milligrams, but in IUs, which is a much smaller dosage. 250mcg or micrograms is equal to 50 IUs or international units. A microgram is 1/1000 of a milligram. The normal dosage of Vitamin D is about 2000 IUs.
 Vitamin C, which most people are already taking in their prenatal vitamins, but maybe a larger dose of 2,000-5,000 mgs. per day. Vitamin C is water soluable so you will pee out whatever is too much for the system. Also, if you are taking too much your body will let you know through loose stools. Do not take anymore that day if this happens. Or, give your body a break and take some later during the day or night.
Vitamin C, which most people are already taking in their prenatal vitamins, but maybe a larger dose of 2,000-5,000 mgs. per day. Vitamin C is water soluable so you will pee out whatever is too much for the system. Also, if you are taking too much your body will let you know through loose stools. Do not take anymore that day if this happens. Or, give your body a break and take some later during the day or night.
Resveratrol (that’s the good stuff in red wine) at about 250 a day.
THere is also another vital vitamin to take a look at and integrate into your supplements this season: Vitamin D Theory (Taken from www.foodconsumer.org)
“…Cannell has reported on Sept 16 in his newsletter that two physicians, one in Wisconsin and the other in Georgia, suggested that vitamin D supplementation can be the key to H1N1 flu prevention.”

“Norris Glick, M.D. of Central Wisconsin Center in Madison, Told Cannell in his email that the 274 residents at his health care facility took vitamin D supplements and where monitored regularly for their plasma vitamin D levels; as a result, only two residents developed influenza-like illness and had positive tests for H1N1 during a period of observation. This compares to 103 of 800 staff members during the same period who were not required for the supplementation. This huge difference may be due likely to use of vitamin D supplements.
 Dr. Ellie Campbell, who also responded to Cannell’s vitamin D theory, told Dr. Cannell in an email of a similar observation. She said she told her patients to take 2,000 to 5,000 IU of vitamin D regularly and monitored their serum levels to make sure her patients had sufficient Vitamin D in their blood. Campbell shared office with another physician. Her office mate did not do the same thing to his patients. When H1N1 hit George, none of her patients came to see her for H1N1 virus infection while the other physician was seeing one to 10 cases per week of influenza-like illness.”
Dr. Ellie Campbell, who also responded to Cannell’s vitamin D theory, told Dr. Cannell in an email of a similar observation. She said she told her patients to take 2,000 to 5,000 IU of vitamin D regularly and monitored their serum levels to make sure her patients had sufficient Vitamin D in their blood. Campbell shared office with another physician. Her office mate did not do the same thing to his patients. When H1N1 hit George, none of her patients came to see her for H1N1 virus infection while the other physician was seeing one to 10 cases per week of influenza-like illness.”
 Not to be too obsessive about this, there’s also hand sanitizer, which is a really good idea. A little bottle in your purse, and then use it whenever you’ve been out anywhere. Most drug stores have the little bottles right by the check-out counter.
Not to be too obsessive about this, there’s also hand sanitizer, which is a really good idea. A little bottle in your purse, and then use it whenever you’ve been out anywhere. Most drug stores have the little bottles right by the check-out counter.

Another thing to do that can help to keep you healthy is nasal gavage. Use a Neti Pot once a day – every day. If you are around someone ill go home and use it. Many doctor’s particularly ENT’s for eye, ear, nose surgery comment, if all their patients used this every day they would be out of business. It helps to rinse all the allergens and germs out of your nasal passage. Learn about it at a local health food store or here online:

It works great! But one caution – you need to use 1/4 t. of sea salt and 1/4 t. baking soda. If you don’t use the baking soda it burns like crazy – the baking soda acts as a buffer. Clean your nostrils at least once every day with warm salt water. Not everybody may be good at Jala Neti or Sutra Neti (very good Yoga asanas to clean nasal cavities), but blowing the nose hard once a day and swabbing both nostrils with cotton buds dipped in warm salt water is very effective in bringing down viral population.

Other ‘nasal washes’ you might look into are: NeiMed Sinus Rinse which one of my pregnant woman says is inexpensive and she uses it in the shower. Get it at a local drug store or online at:
Another, more sophisticated way to keep one’s nasal passages irrigated: Naväge Nasal Hygiene System, the world’s only nasal rinser using controlled light suction to gently wash the nasal passages. Devices like the neti pot and squeeze bottle
push saline through the nose. Doctor recommended Naväge makes the innovative leap to light, powered suction and gently
pulls saline through the nasal cavity. The result is an elegant new way to keep your nose clean. It’s easy to use, convenient, comfortable and safe. And it doesn’t make a mess! Please join us on the road to better nasal health starting today, and begin to enjoyimmediate sinus relief along with the lifelong benefits of superior nasal hygiene.

Other suggestions to help prevent the spread of infection:

– Wash your hands frequently.
– Cover your mouth and nose with a tissue if you sneeze or cough.
– If you eat pork, cook your it thoroughly.
– Avoid travel. If you have any symptoms, stay home.
– If your symptoms are severe, immediately contact your healthcare professional.
“The H1N1 Primer for Pregnant Women” by Maryl Smith
© 2009 Midwifery Today, Inc. All rights reserved.
________________________________________________________________________
Advice regarding breastfeeding for mothers with possible H1N1 infection
Ruth A. Lawrence, M.D., FAAP and John S. Bradley, M.D., FAAP Published on October 13, 2009 AAP News 2009, doi:aapnews.20091012-1 © 2009 American Academy of Pediatrics: http://aapnews.aappublications.org/cgi/content/long/aapnews.20091012-1v1
 Neonates and infants younger than 6 months of age are at risk for complications from seasonal influenza and presumably 2009 H1N1 influenza (swine flu), although the morbidity and mortality from this new virus have not yet been described.
Neonates and infants younger than 6 months of age are at risk for complications from seasonal influenza and presumably 2009 H1N1 influenza (swine flu), although the morbidity and mortality from this new virus have not yet been described.
While the advantages of breastfeeding are well-known, this close interaction of mother and newborn also can facilitate transmission of influenza virus. The benefits and the risks of close contact must be considered carefully.
To protect the infant from possible serious infection while allowing essential and encouraged mother-infant bonding to occur, a compromise is required until more data are available. The following precautions are suggested to minimize the risk of infection to the infant, particularly while still in the hospital and while the mother is symptomatic with fever and coryza:
 – Pay careful attention to handwashing prior to any contact.
– Pay careful attention to handwashing prior to any contact.
– Prior to breastfeeding, wash the breast with mild soap and water; rinse well.
– The mother should wear a surgical mask to prevent nasal secretions and the spontaneous cough or sneeze from inoculating the infant.
– Use clean blankets and burp cloths for each contact.
– Monitor the maternal-infant interaction on perinatal floors for compliance with the above precautions.
– Gargle twice a day with warm salt water (use Listerine if you don’t trust salt). *H1N1 takes 2-3 days after initial infection in the throat/ nasal cavity to proliferate and show characteristic symptoms. Simple gargling prevents proliferation. In a way, gargling with salt water has the same effect on a healthy individual that Tamiflu has on an infected one. Don’t underestimate this simple, inexpensive and powerful preventative method.
– Drink as much of warm liquids (tea, coffee, etc) as you can. *Drinking warm liquids has the same effect as gargling, but in the reverse direction. They wash off proliferating viruses from the throat into the stomach where they cannot survive, proliferate or do any harm.
These precautions are designed to minimize the risk of transmission until mother’s immune response to H1N1 influenza is established, and increased, specific immune protection may be provided by breast milk. Note that influenza virus does not pass through breast milk.
 Although the most effective way to prevent influenza transmission is complete separation from her infant when a mother is receiving antiviral treatment, separation may create more long-term problems in breastfeeding success and mother-infant bonding than any potential benefit achieved from avoiding infection in the newborn infant.
Although the most effective way to prevent influenza transmission is complete separation from her infant when a mother is receiving antiviral treatment, separation may create more long-term problems in breastfeeding success and mother-infant bonding than any potential benefit achieved from avoiding infection in the newborn infant.
For any mother with H1N1 influenza infection who presents in labor to a health care institution, testing and empirically starting therapy for influenza with an antiviral is suggested. Oseltamivir (Tamiflu) or zanamivir (Relenza) will hasten resolution of symptoms and infectivity, particularly if treatment is started within 48 hours of onset of illness. Neonatal exposure to oseltamivir (Tamiflu) excreted in breast milk is extremely low.
Immediately following delivery, the precautions listed above should be instituted as the newborn infant is first placed into mother’s arms. These precautions should be followed until mother’s illness is resolved, i.e., no fever, as measured without antipyretics, for 24 hours.
 While no data exist to support these suggestions, it is believed that these represent an appropriate balance between the benefits of mother-infant interaction and the risks of serious neonatal infection. Institutions may wish to modify of these suggestions to address their needs and medical practices.
While no data exist to support these suggestions, it is believed that these represent an appropriate balance between the benefits of mother-infant interaction and the risks of serious neonatal infection. Institutions may wish to modify of these suggestions to address their needs and medical practices.
Dr. Lawrence is chair of the AAP Section on Breastfeeding executive committee. Dr. Bradley is a member of the AAP Committee on Infectious Diseases.
_______________________________________________________________________
It is very important that you do your own research. Don’t let anyone tell you what to do. This is your body, your life, your children and it is important what ever you choose to do, not to judge someone else for their choice. We are here to learn to agree to disagree. Everyone’s level of development, fear, trust and preventative abilities is different. Don’t just do something bacause someone says it’s the best thing to do. Assume your power by gathering knowledge, going inside and making an informed choice.
| Know the Difference between Cold and H1N1 Flu Symptoms |
|
Symptom
|
Cold
|
H1N1 Flu
|
|
Fever
|
Fever is rare with a cold.
|
Fever is usually present with the flu in up to 80% of all flu cases. A temperature of 100°F or higher for 3 to 4 days is associated with the flu.
|
|
Coughing
|
A hacking, productive (mucus- producing) cough is often present with a cold.
|
A non-productive (non-mucus producing) cough is usually present with the flu (sometimes referred to as dry cough).
|
|
Aches
|
Slight body aches and pains can be part of a cold.
|
Severe aches and pains are common with the flu.
|
|
Stuffy Nose
|
Stuffy nose is commonly present with a cold and typically resolves spontaneously within a week.
|
Stuffy nose is not commonly present with the flu.
|
|
Chills
|
Chills are uncommon with a cold.
|
60% of people who have the flu experience chills.
|
|
Tiredness
|
Tiredness is fairly mild with a cold.
|
Tiredness is moderate to severe with the flu.
|
|
Sneezing
|
Sneezing is commonly present with a cold.
|
Sneezing is not common with the flu.
|
|
Sudden Symptoms
|
Cold symptoms tend to develop over a few days.
|
The flu has a rapid onset within 3-6 hours. The flu hits hard and includes sudden symptoms like high fever, aches and pains.
|
|
Headache
|
A headache is fairly uncommon with a cold.
|
A headache is very common with the flu, present in 80% of flu cases.
|
|
Sore Throat
|
Sore throat is commonly present with a cold.
|
Sore throat is not commonly present with the flu.
|
|
Chest Discomfort
|
Chest discomfort is mild to moderate with a cold.
|
Chest discomfort is often severe with the flu.
|




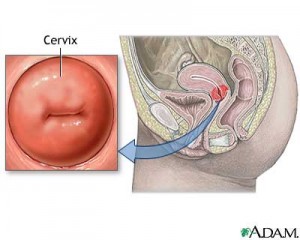 “I think it’s a good and empowering thing for a woman to check her own cervix for dilation. This is not rocket science, and you hardly need a medical degree or years of training to do it. Your vagina is a lot like your nose- other people may do harm if they put fingers or instruments up there but you have a greater sensitivity and will not do yourself any harm.
“I think it’s a good and empowering thing for a woman to check her own cervix for dilation. This is not rocket science, and you hardly need a medical degree or years of training to do it. Your vagina is a lot like your nose- other people may do harm if they put fingers or instruments up there but you have a greater sensitivity and will not do yourself any harm. “The best way to do it when hugely pregnant is to sit on the toilet with one foot on the floor and one up on the seat of the toilet. Put two fingers in and go back towards your bum. The cervix in a pregnant woman feels like your lips puckered up into a kiss. On a non-pregnant woman it feels like the end of your nose. When it is dilating, one finger slips into the middle of the cervix easily (just like you could slide your finger into your mouth easily if you are puckered up for a kiss). As the dilation progresses the inside of that hole becomes more like a taught elastic band and by 5 cms dilated (5 fingerwidths) it is a perfect rubbery circle like one of those Mason jar rings that you use for canning, and about that thick.”
“The best way to do it when hugely pregnant is to sit on the toilet with one foot on the floor and one up on the seat of the toilet. Put two fingers in and go back towards your bum. The cervix in a pregnant woman feels like your lips puckered up into a kiss. On a non-pregnant woman it feels like the end of your nose. When it is dilating, one finger slips into the middle of the cervix easily (just like you could slide your finger into your mouth easily if you are puckered up for a kiss). As the dilation progresses the inside of that hole becomes more like a taught elastic band and by 5 cms dilated (5 fingerwidths) it is a perfect rubbery circle like one of those Mason jar rings that you use for canning, and about that thick.”




 ~
~ When one takes rolaids, it is COUNTER PRODUCTIVE to the absorption of the iron in the body. Rolaids is an ANTACID, (not acidic) and you NEED acid to absorb the iron in your body. So, you are just canceling out the iron supplement each time a rolaid is taken. It doesn’t matter if one takes one or ten…IT IS NOT GOOD! Research shows if a pregnant woman has to choose between chalk and rolaids, the more favorable choice is the chalk. It doesn’t have the antacid element to it. STOP rolaids immediately if your doctor has suggested this as a solution away from the chalk.
When one takes rolaids, it is COUNTER PRODUCTIVE to the absorption of the iron in the body. Rolaids is an ANTACID, (not acidic) and you NEED acid to absorb the iron in your body. So, you are just canceling out the iron supplement each time a rolaid is taken. It doesn’t matter if one takes one or ten…IT IS NOT GOOD! Research shows if a pregnant woman has to choose between chalk and rolaids, the more favorable choice is the chalk. It doesn’t have the antacid element to it. STOP rolaids immediately if your doctor has suggested this as a solution away from the chalk. Floradix is a liquid formula that will help to enhance the iron absorbtion in one’s body when eating iron rich foods.
Floradix is a liquid formula that will help to enhance the iron absorbtion in one’s body when eating iron rich foods. 1. Ferrous Phosphate: 6X or 12X strength, take 1-4 times per day, 4 pellets. This very useful cell salt is known as the “oxygen carrier”. It has the ability to carry oxygen to all the cells of the body for use in conversion to energy.
1. Ferrous Phosphate: 6X or 12X strength, take 1-4 times per day, 4 pellets. This very useful cell salt is known as the “oxygen carrier”. It has the ability to carry oxygen to all the cells of the body for use in conversion to energy. The 12 Tissue/Cell Salt Combination As the name implies, this is a combination of all 12 salts in a single tablet. This combination can be used daily in much the same way as you would take a vitamin or supplement. To treat specific conditions, however, select one of the single salts listed above. RECOMMENDED POTENCY – 6X is the most widely used potency. These are all the different MINERALS combined into the 12 Tissue/Cell Salts.Calcarea Fluoricum Calcarea Phosphoricum Calcarea Sulphuricum Ferrum Phosphoricum Kali Muriaticum Kali Phosphoricum Kali Sulphuricum Magnesia Phosphoricum Natrum Muriaticum Natrum Phosphoricum Natrum Sulphuricum Silicea (Silica)
The 12 Tissue/Cell Salt Combination As the name implies, this is a combination of all 12 salts in a single tablet. This combination can be used daily in much the same way as you would take a vitamin or supplement. To treat specific conditions, however, select one of the single salts listed above. RECOMMENDED POTENCY – 6X is the most widely used potency. These are all the different MINERALS combined into the 12 Tissue/Cell Salts.Calcarea Fluoricum Calcarea Phosphoricum Calcarea Sulphuricum Ferrum Phosphoricum Kali Muriaticum Kali Phosphoricum Kali Sulphuricum Magnesia Phosphoricum Natrum Muriaticum Natrum Phosphoricum Natrum Sulphuricum Silicea (Silica) Spinach is a source of non-heme iron, which is usually found in vegetable sources. Unlike heme iron found in animal products, non-heme iron is not as bioavailable to the body.
Spinach is a source of non-heme iron, which is usually found in vegetable sources. Unlike heme iron found in animal products, non-heme iron is not as bioavailable to the body.

 ~
~ Of course, I am in favour of the abolition of electronic fetal monitoring but it would be far more uplifting if this was being done for some sort of health improvement and not just more ways to cover butt in court.
Of course, I am in favour of the abolition of electronic fetal monitoring but it would be far more uplifting if this was being done for some sort of health improvement and not just more ways to cover butt in court. One of the midwife “tricks” that we were taught was to ask the mother’s shoe size. If the mother wore size five or more shoes, the theory went that her pelvis would be ample. Well, 98 percent of women take over size five shoes so this was a good theory that gave me confidence in women’s bodies for a number of years. Then I had a client who came to me at eight months pregnant seeking a home waterbirth. She had, up till that time, been under the care of a hospital nurse-midwifery practise. She was Greek and loved doing gymnastics. Her eighteen-year-old body glowed with good health, and I felt lucky to have her in my practise until I asked the shoe size question. She took size two shoes. She had to buy her shoes in Chinatown to get them small enough—oh dear. I thought briefly of refreshing my rusting pelvimetry skills, but then I reconsidered. I would not lay this small pelvis trip on her. I would be vigilant at her birth and act if the birth seemed obstructed in an unusual way, but I would not make it a self-fulfilling prophecy. She gave birth to a seven-pound girl and only pushed about twelve times. She gave birth in a water tub sitting on the lap of her young lover and the scene reminded me of “Blue Lagoon” with Brooke Shields—it was so sexy. So that pelvis ended the shoe size theory forever.
One of the midwife “tricks” that we were taught was to ask the mother’s shoe size. If the mother wore size five or more shoes, the theory went that her pelvis would be ample. Well, 98 percent of women take over size five shoes so this was a good theory that gave me confidence in women’s bodies for a number of years. Then I had a client who came to me at eight months pregnant seeking a home waterbirth. She had, up till that time, been under the care of a hospital nurse-midwifery practise. She was Greek and loved doing gymnastics. Her eighteen-year-old body glowed with good health, and I felt lucky to have her in my practise until I asked the shoe size question. She took size two shoes. She had to buy her shoes in Chinatown to get them small enough—oh dear. I thought briefly of refreshing my rusting pelvimetry skills, but then I reconsidered. I would not lay this small pelvis trip on her. I would be vigilant at her birth and act if the birth seemed obstructed in an unusual way, but I would not make it a self-fulfilling prophecy. She gave birth to a seven-pound girl and only pushed about twelve times. She gave birth in a water tub sitting on the lap of her young lover and the scene reminded me of “Blue Lagoon” with Brooke Shields—it was so sexy. So that pelvis ended the shoe size theory forever.


 ~
~